Don's gem's Jan-Feb 02
The Wizard's potion
These are some of Don's interesting comments from the Friday morning case conferences. Any errors in this section are solely the poor recording of otherwise accurate comments, due to the pressure of the quantity of interesting comments. This section is updated weekly.
This section has outgrown it's page and been subdivided. Previous sections are linked below.
| 2001 | July | August | September | October | November | December | ||||||
| 2002 | Jan | Feb | March | April |
Febuary 22nd 2002 Scripps
1. Inflammatory OA can cause fusions. It is a continuum with OA.
2. Nutrient foramina of fingers can be enlarged in sarcoidosis and sickle cell disease, but are not enlarged in inflammatory OA.
3. Pseudogout can also produce tophaceous masses.
4. OA shoulders; consider: Trauma, Occupational, Crystals-CPPD,HA, AVN, Epiphyseal dysplasia, Acromegaly, Ochronosis, Ankylosing spondylitis.
5. Ankylosing spondylitis involves the root joints, hips and shoulders. The "Elizabethian ruff" collar of osteophytes on the femoral head is suggestive but not diagnostic.
6. Myeloma lytic lesions can have a calcified centre. Looks like apthous ulcers on Ba. Possibly healing, dystrophic in necrotic centre, or related to amyloid deposition. Healing lesions more commonly have sclerotic margins.
7. Generalised increase in bone density: Mets, Pagets, Fluorosis, ROD, Myelofibrosis, Mastocytosis.
8. PVNS presents relatively early at the hip compared to other joints, due to the tightness of the capsule.
9. Ollier's can be associated with a chondral channel through the bone. In smaller bones the enchondromas can protrude.
10. The malignancy in Maffucci's can be bone or ST.
11. Retin A treatment for acne can cause a premature bone bar across the physis, and premature fusion.
12. The volar extrinsic radiocarpal ligaments include the radioscaphocapitate and radiolunotriquetral. There may possibly be a volar recess to the radiocarpal overlying the volar aspect of the scapholunate joint.
13. Traumatic bowing deformity usually occurs in long bones that are already physiologically bowed due to axial (longitudinal) loading. ie tibia and radius.
14. Osteopoikilosis tends to be ovoid and metaphyseal.
15. Melorrheostosis is related to linear scleroderma, which is a localised skin condition not related to systemic sclerosis.
Febuary 15th 2002
1. Plantar fibromatosis is usually on the medial aspect of the central band. Fibrous tissue is even low on T2FS. Can look aggressive, but most become quiescent.
2. Xanthoma of the achilles tendon produces a stippled signal change.
3. Posteromedial oedema at the knee. Above the joint consider injury to the posterior oblique ligament. Below the joint line consider semimembranosis tendon.
4. If the posterolateral corner is incompetent then an ACL repair will likely fail.
5. There is an increased risk of arthrofibrosis if an ACL tear is treated acutely. Arthrofibrosis to an orthopod is equivalent to stiff.
6. Extracapsular ligaments heal better than intracapsular ligaments.
7. Lucky strike means fine tobacco. Liposclerosing mixed fibrous tumour of bone. This one was a doughnut lesion, which means sclerotic rim with lucent centre. 10-16% malignant transformation (AFIP) but probably lower. DDx fibrous dysplasia and involuting intraosseus lipoma.
8. DISH of Cx < Tx spine. Lucent areas between body and new bone. DDx DASH due to retinoids. DISH greatest C4-C7. DASH upper Cx spine. Outgrowth anterior C1 distinctive for DASH. DISHphasia is rare, so consider Ca oesphagus. Anterior vertebral body scalloping seen in long standing Ank Spond is not seen in DISH.
9. Volkmann's ischaemic contracture is a missed compartment syndrome, in which the pulses are the last thing to go. Pressures measured with a wick catheter. This can produce the anterior interosseous syndrome, which is a branch of the median nerve adjacent to the membrane. This is also known as the Kelo Nevin syndrome. Muscles involved are adjacent to the membrane and include FDP, PT, FDS, FCU. Sometimes there is an anastomosis between the median and ulna nerves, called the Martin Gruber anastomosis, to form the AIN.
10. Longitudinal splits of the tibialis posterior tendon are more common with a cornuate navicular.
11. Peroneus brevis should not be lateral to peroneus longus, if so then torted.
12. Thickening of the anterior talofibular ligament is equivalent to anterior impingment syndrome.
13. The accessory peroneus quartis is associated with peroneus brevis splits. It seperates off the side of PB and attaches to the calcaneus. 30% of PB splits have associated PL splits.
14. In 1952 Michael Pitt described synovial pits on the anterior femoral neck. They are thought to be reactive bony changes to overlying fasciitis of iliopsoas tendon on capsule.
Febuary 5th 2002 Mini
1. Cervical vertebral body sagittal plane fractures occur with axial loading. May affect consecutive levels.
2. High signal in the cord on T1 indicates haemorrhage and a worse prognosis than just oedema.
3. A valsava can be used to open up the airway to assess prevertebral STS.
4. Due to muscle spasm a posterior ST injury that produces a flexion subluxation injury, may not show on flexion views for 2/52.
5. An injury to an already fused cervical spine causes more paravertebral haemorrhage,
6. Hangman Fx. Effendi classification
Grade 1: extension injury, displacement < 2mm. Rx flexion.
Grade 2: extension injury, displacement >2mm and angulation. Rx flexion.
Grade 3: flexion injury, C2-3 facet joint subluxation/dislocation. Rx extension.
20% of hangman Fxs extend into body of C2, associated with vertebral artery occlusion.
7. Horizontal fractures occur in the fused spine.
8. Tear drop Fxs of the upper Cx spine are extension and lower Cx spine and flexion .
9. Most flexion tear drop Fxs have a sagittal component.
Febuary
1st 20021. Due to the shape of the meniscus, with a flat inferior margin and curved superior margin, the lower meniscotibial ligament is more important for stability of the meniscus than the upper meniscofemoral portion of the deep part of the MCL.
2. TFC tears are more likely with RhA than with gout.
3. Tendon ossification occurs with chronic trauma and degeneration. It is most common in the achilles and the quads.
4. The FHL tendon sheath communicates with the ankle in 20%.
5. Fluid fluid level in a bone lesion: ABC, SBC, GCT, telangiectatic OS.
6. SBC occur in tubular bones in children and flat bones of adults.
7. ST Haemangioma; regresses, high flow, poorly marginated, can have areas of fat, lined by endothelium.
8. Venous malformation; slow flow, fluid level in sinusoids, can have calcifications
Vascular malformations; 4 types
High flow, Haemangioma in child - resolves, don't treat.
AVM - don't resolve. i.e. Klippel Trenauney Webber, infact grow.
Low flow, Venous malformations - slow flow, phleboliths, fluid/fluid levels
Lymphangiomas
9. A labral injury is an important part of the posterosuperior impingement syndrome, as well as the undersurface fraying and the greater tuberosity cystic change.
January 25th 2002
1. A band of subchondral sclerosis may be a marker of heamachromatosis.
2. ACJ seperation grading.
1. ACJ lig sprain with minimal change in height.
2. ACJ lig tear with widened joint.
3. Clavicle 1 bone width superiorly displaced, disrupted CC ligs.
4. As above with posterior displaced clavicle.
5. As 3, with marked superior displacement.
6. Inferiorly displaced clavicle, either subacromial or subcoracoid.
A Bosworth screw is used to fix the coracoid to the acromium for CC lig disruption.
3. A bland knee effusion on MRI has well defined margins and usually indicates trauma or internal derangement. A proliferative effusion has ill defined margins and occurs in the inflammatory arthritides and with synovial proliferative conditions.
4. Juxta articular lymphadenopthy is seen more commonly in JRA > RhA > other arthritides.
5. RhA is associated with secondary septic arthritis.
6. RhA is the leading cause of polyarticular septic arthritis.
7. Muscle strain grading.
1. Increased signal.
2. Fluid collection with architechtural disturbance.
3. Complete disruption.
8. Sourcil is a French word for eyebrow and refers to the superolateral aspect of the acetabulum.
9. Ganglion cysts are filled with thick mucinous material which has fluid signal on MRI. They have a collagen border, but unlike non-communicating synovial cysts, no proper capsule. Freda Feldman wrote a good article in the 70s.
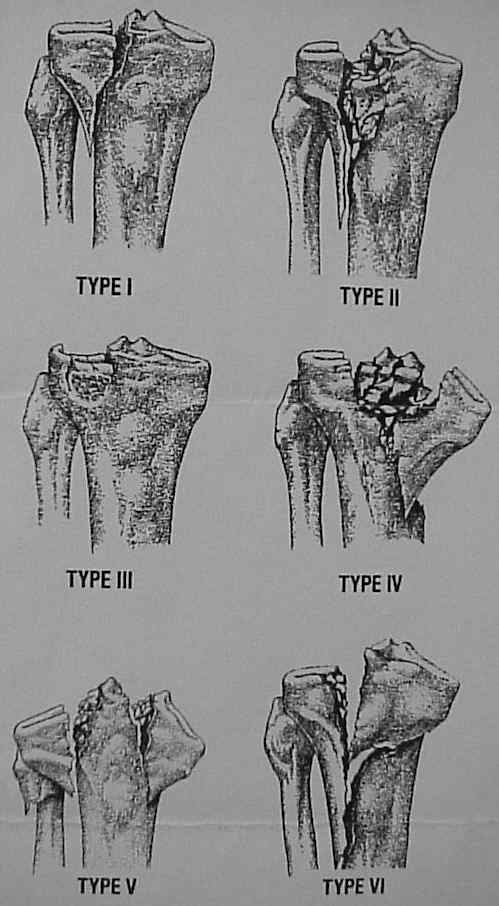
10. Tibial plateau fractures are best assessed with MRI for the acccopanying ST injuries, with adequate visualisation of the fractures. Tibial plateau fractures are classified by the Schatzker classificaion. 1. lateral split. 2. split with depression. 3. pure lateral depression. 4. pure medial depression. 5. bicondylar. 6. split extends to metadiaphyseal region. Type 2 most commonly associated with MCL inj. Type 4 most commonly associated with MM injuries. MR is better than CT for the accompanying ST injuries, but CT has higher resolution for the fracture fragments. 2mm max articular displacement in center of excellence and 4mm in country practice.
11. TMJ MRI. Standard sequence is Sag T1, but GRE T2* look good. In the closed mouth position the posterior aspect of the disc should be within 10 degrees of the 12 O'clock location on the condyle. Open mouth the disc should relocate so that the condyle lies centrally in the biconcave disc. The disc is like an intervertebral disc and has proteoglycans centrally like a nucleus pulposes. Problems maybe related to adhesions of the posterior band. "possibly a diseasse of the developed world, due to a lack of chewing gum in Mogadishu"
12. There is an anterior glenoid notch at approximately 2 O'clock. This can have a bow string effect on the labrum and a consequent sublabral hole.
13. Subtalar coalition. Can be fibrous, cartilaginous or bony. Talocalcaneal and calcaneonavicular the most common. The subtalar joint is divided into anterior and posterior joints, or 3 facets, with the posterior facet being the posterior joint, and the anterior joint (talocalcaneonavicular) made up of the anterior facet (talonavicular) and middle facet (sustentaculum talus/talus J). The anterior and middle facets always communicate. The middle and posterior facets are separated by the tarsal canal continuation of the tarsal sinus. Talocalcaneal coalition usually involves the middle facet. Talocalcneal coalition of the posterior facet is rare and when present is at the anterior medial aspect of the joint. Bone scan is often hot around the coalition, even if a solid bony coalition.
January 18th 2002 Rheumatology
1. RhA occasionally sparres the 4th MCPJ
2. If Ankylosing spondylitis fuses the facets early, then they will often not develop body syndesmophytes.
3. With oblique views of the feet, there can be a normal notch on the medial aspect of the MT heads, which should not be mistaken for erosion.
4. AVN of the humeral heads can appear as just a snow cap appearance.
January 18th 2002
1. Signs of meniscal instability:
1. Fluid signal on T2, careful with FS images.
2. Displaced.
3. Lesion greater than 10mm in both planes.
4. Greater than one cleavage plane.
2. A meniscal flounce is a concertina appearance to the meniscal body inner margin. It is a positional variation of the meniscus. It can be associated with ligament injuries, ACL or MCL. It is possibly related to the semimembranosus attachments and may well go on flexion.
3. Leaking para knee cysts can mimic MCL tears with fluid around the MCL.
4. An injury to the oblique arm of the semimembranosis tendon is a significant injury.
5. Pelligrini Stieda lesion can involve either the proximal MCL or the Adductor magnus insertion.
6. Cystic angiomatosis can appear as multiple discrete lesions with sclerotic rims. Often the sclerotic margins can be thick and occasionally may completely fill in. On MRI they are high signal on T2 and low on T1. Schweitzer described the bull's eye as a lesion seen on T1 with high signal centre and low signal periphery. This is a negative predictive sign for a met. He also described the halo on T2 imaging as low centre and high periphery as a positive predictor for mets.
7. Spontaneous tapering of the lateral navicular into a coma shape is the Mueller Weiss syndrome. It is often bilateral and asymmetric. Can be related to underlying diabetes or CRF. It is possibly stress related. It is different from Kohler's which causes a disc like collapse in chilren which recovers.
8. 90% of segond Fxs have an ACL tear.
10% of ACL tears have a segond Fx.
NAVY CONFERENCE.
16th of January/Dr Don Resnick
OO are most commonly located in the femur and tibia and MRI can detect them depending how close they are to the medullary cavity. Mini asked whether the drugs that are taken (salicyclates) affect the edema pattern.
DR then showed a very interesting case of an AP and medial oblique ankle, with thickening of the distal fibula cortex with a complementary periostitis along the abutting tibial surface. If an OO is located in the long bone or a bone which is adjacent to another, then it likes to induce a periostitis in the adjacent bone.
CT in OO can demonstrate a large nidus for the size of the original cortex which is somewhat surprising. MRI can show dramatic edema in the soft tissue and marrow. OO can mimic or simulate tumors or infection so CT is the preferable modality of choice. OO treatment is with percutaneous ablation though this is not being used all that much here at the moment.
Teaching Points. – Multifocal OO can occur and if the nidus is not removed, then the OO may recur. OO have no malignant potential.
Also remember that when an OO is in a joint,(most commonly the hip), then it may just invoke a synovitis which is important since this will induce early degenerative joint disease.
Note should also be made that Brodies abcesses are only very rarely seen in comparison to OO.
The abnormality was noted in the posterior aspect of the distal femur, with flecks of calcification being noted to be located in a disorganized manner. The differential includes intra-articular chondromas, bodies in a synovial cyst, soft tissue tumors (seen (in younger patients) and crystal deposition diseases (HADD and CPPD)
Patients with CPPD have articular cartilage calcification, but also have it elsewhere ie synovial calcification and capsular (the elbow, metacarpals and metatarsals are the most common sites) and tendons of which the most common is the Achilles, gastroc’s, and quads as well as possibly the rotator cuff. It is not known if the medial or the lateral head of the gastoc’s is the more common location to find the crystal depoition. Calcification in the gastoc’s may be a manifestation of CPPD, as with this patient who did not have any trauma.
MRA is often needed to make a couple of observations;. Remember that in young people histologically the tendon is attached right across the facets whereas in older patients there may be peeling off from the medial margin of the tuberosity, which is not a tear.
Note that there is contrast in the SS medial to its’ substance and recognising when it is an undersurface tear in SS and IS with contrast under the muscle with partial and also complete tears. The anterior labrum – continues here between the anterior inferior labrum and the glenoid in the axial image and an ABER is needed for the diagnosis.
ABE’Rs are good for evaluating the undersurface of the rotator cuff (true; ABER is great for partial undersurface cuff tears) and also the labrum when it is lifted off which is the most subtle pattern of labral injury
An 86 year old female from Scripps.
The anterior band of the inferior gleno-humeral complex – look at the humerus and the glenoid site of insertion since there may be disruption of the humeral band with leaking of material under the capsule. This may be seen with a partial subscapularis tear, luxatio erecta and in older patients. Remember that also a posterior HAGEL (HAGL- humeral avulsion of glenohumeral ligament- usually the inferior one) may be associated with a avulsion of the triceps.
4) A hypoplastic glenoid or denticulate glenoid which may be overdiagnosed on oblique projections and may be associated with mild hypoplasia of the humeral head and acromion. MRI may be helpful in showing the bulbous posterior labrum and the labrum may develop away from the glenoid labrum. The glenoid labrum ovoid mass is an associated term (GLOM)
Mohammed talked about MRA, which had shown that as well as the bony hypoplasia, that there may be also abnormal tissue posterior which may represent hypertrophied synovial tissue and with gadolinium, showed that there was indeed tracking of this through the substance of the tissue implying ulceration but this was not proven. DR commented that he had done plain film radiography, which showed channels of contrast tracking.
1) Cystic adventitial disease (CAD)
2) Popliteal artery entrapment syndrome. (PAES)
Angiography shows thrombosis in the popliteal artery and with longstanding entrapment, there is a large geniculate artery and geniculate collaterals. The differential may be difficult especially without the supporting history!
The artery is most often affected and presents in 50% of cases with a thrombosis. Without this it may be difficult to diagnose but the popliteal artery may be deviated medially. On the T2 fat sat images, the artery sits lateral to the insertion of the medial head of the gastroc’s. The wall of the artery needs to be assessed and in the entrapment syndrome, this is normal and therefore is not CAD. So then one must look for the location of the vascular structures. The artery should lie medial to the vein and both should run about in the midline to the femur and the popliteal artery should lie lateral to the head of the medial head of the gastoc’s. It should not insinuate it, as in this case, and here it is seen to lie medial to the medial head and is therefore clearly abnormal.
There are 4 distinct types of PAES:
The popliteal vein may follow the artery which occurs in 10%
The anatomy is normal but there is functional entrapment i.e. in athletes where they get hypertrophy of the gastroc’s.(This is sometimes referred to as Type VI)
Mikes case was that of a Type 1. He also said that there is no case of an abnormality in the popliteal vein without a concomitant abnormality in the artery because of how the artery forms embryologically.
Another case of claudication weas shown this time with a normal arterial wall and the course of the artery was normal and in the mid-line. Here there is an abnormal relationship between the medial head of the gastoc’s and a small slip of muscle and the entrance of the popliteal artery and vein. A little dot on the coronal T1 images represented the accessory slip and this was therefore a type 3.
The last case that was shown in this series was that of a 35-year old male with right lower extremity claudication. The arterial wall of the popliteal artery was clearly abnormal at the level of the knee with cysts collecting in this region as well as interestingly, cysts connecting to the knee joint via channels. This is the only area where CAD affects – is it to do with the embryology/function /anatomy of the knee joint? Gad introduced intra-articluar ollected in the cysts.
An artery has 3 layers, a medial, or intima layer which is the endothelial layer – the middle or media layer which contains the muscular layer and then the outer or adventitial layer which is the strongest layer of the artery and in this CAD there is a mucin collection in the adventitia and may relate to cystic degeneration and the syndrome is specific to the popliteal artery or maybe it is due to the nerve supply to this region following a Belgium article that was recently published. No exercise or delayed images to the joint where performed but maybe this is something to consider in the future. It may somehow relate to meniscal cysts. One of the Navy medics asked about dynamic imaging and also calf compression. Another comment from the floor was also to include a case of asymmetrical CAD, which may have been a forme fruste.
However it is vital to diagnose this condition because surgically, if it is picked up early then a myotomy is done but if left until late when a thrombosis has formed or injury to the vessel has occurred, it is a much more lengthy procedure and all the patients have to have a vein graft. CAD occurs bilaterally in 15- 20% of cases.
The Virginia case that was shown was that of an ACL repair with no fibres in the graft tunnel and grey material "pouched" out from the anterior surface of the tibia and high signal noted extending into the soft tissue into the anterior tibia. Cystic degeneration of the ACL graft - DR has 5 cases. The femoral tunnel component is less commonly involved being one of the 5 cases that DR has, the others being tibial.
The 4 in the tibia may occur with a ganglion in the soft tissues anterior, and with the cystic degeneration of the graft most commonly with tibia or there may also be osteomyelitis of the graft. Failure of the graft may also occur due to the windshield wiper effect due to the torque. There may also be widening of the tunnel and the ddx is metal artifact which can really cause problems.
A well demarcated, slightly expansile lesion in the region of the lateral femoral condyle with well defined sclerotic borders and a slightly septated center in a younger patient is presented with CT findings to show the cartilaginous nature to the internal matrix and also to show that the cortex is intact throughout its entirety. The signal on T2 is low and the ddx is chondroblastoma, or GCT (or clear chondrosarcoma or not really a healing NOF). This was a chondroblastoma and there was lots of marrow edema! (this finding makes it more likely that the lesion is a chondroblastoma vs a GCT, though Don has shown us cases of both with surrounding edema- i.e. there are no always/nevers in medicine)
January 11th 2002.
1. Muscle tears;
Grade 1. few fibres torn.
2. tearing, loss of function and gap.
3. complete.
2. Muscles crossing 2 joints are more prone to injury.
3. Charlie horse (a frog punch) and a hip pointer (pain at the hip on direct fall) (quote SR) are direct blows with contusions.
4. PCL tears are usually incomplete and stretch. Associated marrow oedema is variable due to a wide range of mechanisms, and is most often anterior tibia.
5. Carpal tunnel syndrome is associated with Tinnel's sign and the Phalen manouver which is flexion for 1 min causing numbess.
6. Fibrolipomatous hamartoma of the median nerve has stippled signal from low signal fascicles and high signal fat.
7. Little league shoulder. Widening of the proximal humeral physis compatible with a Salter Harris 1. Rx rest. Similar to gymnasts wrists. DDx healing rickets or osteomalacia.
8. There is a theory that osteoarthritis may be secondary to tiny occult subchondral fractures. These may be insuffiency. Similarly SONK.
9. The Mitchell classification of AVN on MRI is of little use.
10. PVNS can be diffuse or localised nodular. Pigmented, little pigmented or not pigmented. Villous or nodular or both.
11. Liposclerosing mixed fibrous tumour of bone could be an involuting lipoma. There is possibly a low frequency of malignant degeneration.
12. Ischaemic lower leg in a young person. Cystic adventitial disease of the artery v's entrapment at the knee. There are 4 kinds of popliteal entrapment;
1. Normal gastrocnemius insertion, but artery passes posterior to muscle.
2. Medial head originates laterally.
3. Abnormal slips.
4. Popliteal muscle
Needs surgical correction.
January 4th 2002
1. Lateral process of talus fractures account for 15% of snowboard ankle injuries, but are otherwise rare. They occur with dorsiflexion and inversion of the hind foot. They are less common with the newer hard boots.
2. Osteochondromas are often sessile anteriorly and pudunculated posteriorly at the knee. Although they usually point away from the joint, they arre not tug lesions. Anterior ones may interfere with patella tracking. If the medullary continuity cannot be seen the differential would include an ossified sub periosteal haematoma. They stop growing when the nearby growth plate closes. The cartilage cap can disappear in adults.
3. Intraosseus pneumatocysts are most commonly seen in the spine (particularly Cx) and about the sacroiliac joints. They are likely degenerative or ganglion cysts with a vacuum.
4. Subperiosteal osteoid osteomas are likely common. Rx will depend on location and visibility on plain films. Options include excision, radiographic localisation and excision, scintigraphic localisation and excision, radiofrequency ablation, radiographic guided excision.
5. Lateral epicondylitis (tennis), medial (golf). Rx steroids, rest, release of ECRB.
6. The lateral sesamoid at the 1st MTPJ is in the FHB tendon. It is within the joint and affected by all types of joint disease. The medial is in the abductor hallucis and the FHL passes between them.
7. Synovial sarcoma occurs in the young 15-30 Y age group. Only 10 % are in joints. Although associated with calcification, only 30% calcify, but this is high compared to other ST tumours. DDx includes clear cell sarcoma of tendons and aponeuroses, which contains melanin and is hitologicaly similar to malignant melanoma, but behaves like a sarcoma.
8. Carpal tunnel syndrome, the bowing of the retinaculum is best seen at the level of the hamate, not the pisiform. Signal increased on T2 classically. Be careful with FS since normal nerve much brighter.
9. Distal biceps tendon rupture accounts for only 3% of biceps tendon ruptures. Slingshot rupture is when both the proximal heads rupture and they catapult into the anterior forearm.